 |
| Photo: Reuters |
"SuperBug": NDM1 New Delhi Metallo-beta-lactamas
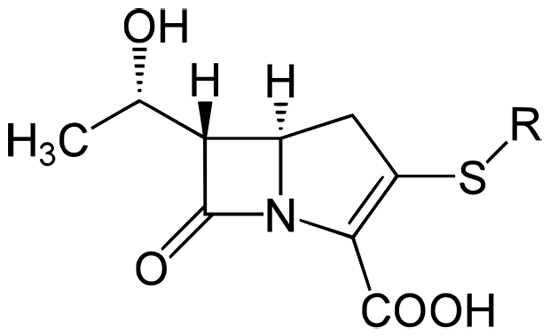
New Delhi Metallo-beta-lactamase (NDM-1) is an enzyme which makes bacteria resistant to a broad range of beta-lactam antibiotics. This includes antibiotics of the carbapenem family, which are a mainstay for the treatment of antibiotic-resistant bacteria. The gene for NDM-1 is one member of a large gene family that encodes beta-lactamase enzymes called carbapenemases. Bacteria which carry such genes are often referred to in the news media as "superbugs", since infections with these bacteria are very hard to treat successfully. Indeed, the United Kingdom Health Protection Agency has stated that "most isolates with NDM-1 enzyme are resistant to all standard intravenous antibiotics for treatment of severe infections." Structure of the carbapenem backbone NDM-1 was first identified in December 2009 in a patient hospitalised in New Delhi with a Klebsiella pneumoniae infection. It has since been detected in bacteria in India, Pakistan, the United Kingdom, the United States, and Canada. The most common organisms expressing this enzyme are the Gram-negative bacteria Escherichia coli and Klebsiella pneumoniae, but the gene for NDM-1 can spread from one strain of bacteria to another through horizontal gene transfer.Carbapenems are a class of beta-lactam antibiotics which are capable of killing most bacteria by inhibiting the synthesis of one of their cell wall layers. The carbapenems were developed to overcome antibiotic resistance mediated by bacterial beta-lactamase enzymes. However, the blaNDM-1 gene produces NDM-1, which is a carbapenemase beta-lactamase ? an enzyme that hydrolyzes and inactivates these carbapenem antibiotics. Carbapenemases are particularly dangerous resistance mechanisms, since they can inactivate a wide range of different antibiotics.The NDM-1 enzyme is one of the class B metallo-beta-lactamase; other types of carbapenemase are class A or class D beta-lactamases. (The class A Klebsiella pneumoniae carbapenemase (KPC) is currently the most common carbapenemase, which was first detected in North Carolina, USA, in 1996 and has since spread worldwide. A later publication indicated that Enterobacteriaceae that produce KPC were becoming common in the United States.) The resistance conferred by this gene (blaNDM-1) therefore aids the expansion of bacteria that carry it throughout a human host, since they will face less opposition/competition from populations of antibiotic-sensitive bacteria, which will be diminished by the original antibacterial treatment. Antibiotic resistance is a type of drug resistance where a microorganism is able to survive exposure to an antibiotic. Genes can be transferred between bacteria in a horizontal fashion by conjugation, transduction, or transformation. Thus a gene for antibiotic resistance which had evolved via natural selection may be shared. Evolutionary stress such as exposure to antibiotics then selects for the antibiotic resistant trait. Many antibiotic resistance genes reside on plasmids, facilitating their transfer. If a bacterium carries several resistance genes, it is called multiresistant or, informally, a superbug.
The primary cause of antibiotic resistance is antibiotic use both within medicine and veterinary medicine. The greater the duration of exposure the greater the risk of the development of resistance irrespective of the severity of the need for antibiotics. The widespread use of antibiotics both inside and outside of medicine is playing a significant role in the emergence of resistant bacteria. Antibiotics are often used in rearing animals for food and this use among others leads to the creation of resistant strains of bacteria. In some countries antibiotics are sold over the counter without a prescription which also leads to the creation of resistant strains. In supposedly well-regulated human medicine the major problem of the emergence of resistant bacteria is due to misuse and overuse of antibiotics by doctors as well as patients. Other practices contributing towards resistance include the addition of antibiotics to the feed of livestock. Household use of antibacterials in soaps and other products, although not clearly contributing to resistance, is also discouraged (as not being effective at infection control). Also unsound practices in the pharmaceutical manufacturing industry can contribute towards the likelihood of creating antibiotic resistant strains.
Certain antibiotic classes are highly associated with colonisation with superbugs compared to other antibiotic classes. The risk for colonisation increases if there is a lack of sensitivity (resistance) of the superbugs to the antibiotic used and high tissue penetration as well as broad spectrum activity against "good bacteria". In the case of MRSA, increased rates of MRSA infections are seen with glycopeptides, cephalosporins and especially quinolones.In the case of colonisation with C difficile the high risk antibiotics include cephalosporins and in particular quinolones and clindamycin. The volume of antibiotic prescribed is the major factor in increasing rates of bacterial resistance rather than compliance with antibiotics. A single dose of antibiotics leads to a greater risk of resistant organisms to that antibiotic in the person for up to a year. Inappropriate prescribing of antibiotics has been attributed to a number of causes including: people who insist on antibiotics, physicians simply prescribe them as they feel they do not have time to explain why they are not necessary, physicians who do not know when to prescribe antibiotics or else are overly cautious for medical legal reasons. A third of people for example believe that antibiotics are effective for the common cold and 22% of people do not finish a course of antibiotics primarily due to that fact that they feel better (varying from 10% to 44% depending on the country). Compliance with once daily antibiotics is better than with twice daily antibiotics.Sub optimum antibiotic concentrations in critically ill people increase the frequency of antibiotic resistance organisms. While taking antibiotics doses less than those recommended may increase rates of resistance, shortening the course of antibiotics may actually decrease rates of resistance. Role of other animals Drugs are used in animals that are used as human food, such as cows, pigs, chickens, fish, etc., and these drugs can affect the safety of the meat, milk, and eggs produced from those animals and can be the source of superbugs. For example, farm animals, particularly pigs, are believed to be able to infect people with MRSA. The resistant bacteria in animals due to antibiotic exposure can be transmitted to humans via three pathways, those being through the consumption of meat, from close or direct contact with animals, or through the environment. The World Health Organization concluded that antibiotics as growth promoters in animal feeds should be prohibited (in the absence of risk assessments). In 1998, European Union health ministers voted to ban four antibiotics widely used to promote animal growth (despite their scientific panel's recommendations). Regulation banning the use of antibiotics in European feed, with the exception of two antibiotics in poultry feeds, became effective in 2006. In Scandinavia, there is evidence that the ban has led to a lower prevalence of antimicrobial resistance in (non-hazardous) animal bacterial populations. In the USA federal agencies do not collect data on antibiotic use in animals but animal to human spread of drug resistant organisms has been demonstrated in research studies. Antibiotics are still used in U.S. animal feed - along with other ingredients which have safety concerns. Growing U.S. consumer concern about using antibiotics in animal feed has led to a niche market of "antibiotic-free" animal products, but this small market is unlikely to change entrenched industry-wide practices. In 2001, the Union of Concerned Scientists estimated that greater than 70% of the antibiotics used in the US are given to food animals (e.g. chickens, pigs and cattle) in the absence of disease.In 2000 the US Food and Drug Administration (FDA) announced their intention to revoke approval of fluoroquinolone use in poultry production because of substantial evidence linking it to the emergence of fluoroquinolone resistant campylobacter infections in humans. The final decision to ban fluoroquinolones from use in poultry production was not made until five years later because of challenges from the food animal and pharmaceutical industries.Today, there are two federal bills S.549and H.R. 962 aimed at phasing out "non-therapeutic" antibiotics in US food animal production.
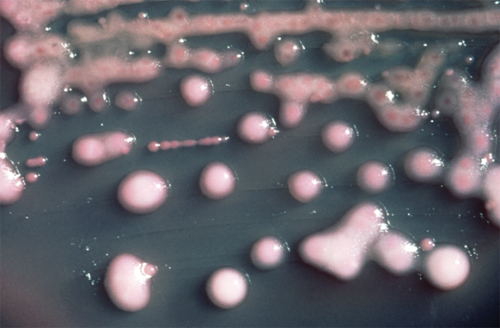 | New Delhi Metallo-beta-lactamase (NDM-1)
(Klebsiella pneumoniae, the bacterium in which NDM-1 was first identified.) |
Origin and spread The NDM-1 enzyme was named after New Delhi, the capital city of India, as it was first described by Yong et al. in December 2009 in a Swedish national who fell ill with an antibiotic-resistant bacterial infection that he acquired in India.The infection was unsuccessfully treated in a New Delhi hospital and after the patient's repatriation to Sweden, a carbapenem-resistant Klebsiella pneumoniae strain bearing the novel gene was identified. The authors concluded that the new resistance mechanism "clearly arose in India, but there are few data arising from India to suggest how widespread it is." In March 2010 a study in a hospital in Mumbai found that the majority of carbapenem-resistant bacteria isolated from patients carried the blaNDM-1 gene. In May 2010 a case of infection with E. coli expressing NDM-1 was reported in Coventry in the United Kingdom. The patient was a man of Indian origin who had visited India 18 months previously, where he had undergone dialysis. In initial assays the bacteria was fully resistant to all antibiotics tested, while later tests found that it was susceptible to tigecycline and colistin. The authors warned that international travel and patients' use of multiple countries' healthcare systems could lead to the "rapid spread of NDM-1 with potentially serious consequences". As of June 2010, there were three reported cases of Enterobacteriaceae isolates bearing this newly described resistance mechanism in the US, the CDC stated that "All three U.S. isolates were from patients who received recent medical care in India." However, US experts have stated that it is unclear if this strain is any more dangerous than existing antibiotic-resistant bacteria such as methicillin-resistant Staphylococcus aureus, which are already common in the USA. Structure of colistin, one of the few antibiotics able to treat NDM-1 positive bacterial infections. In July 2010 a team in New Deli reported a cluster of three cases of Acinetobacter baumannii bearing blaNDM-1 that were found in the intensive care unit of a hospital in Chennai, India in April 2010. As previously, the bacteria were fully resistant to all the aminoglycoside ?-lactam and quinolone antibiotics, but were susceptible to tigecycline and colistin. This particularly broad spectrum of antibiotic resistance was heightened by the strain bearing expressing several different resistance genes in addition to blaNDM-1. A study by a multi-national team was published in the August 2010 issue of the journal The Lancet Infectious Diseases. This examined the emergence and spread of bacteria carrying the blaNDM-1 gene. This reported on 37 cases in the United Kingdom, 44 isolates with NDM-1 in Chennai, 26 in Haryana and 73 in various other sites in Pakistan and India. The authors' analysis of the strains showed that many carried blaNDM-1 on plasmids, which will allow the gene to be readily transferred between different strains of bacteria by horizontal gene transfer. All the isolates were resistant to multiple different classes of antibiotics, including beta-lactam antibiotics, fluoroquinolones, and aminoglycosides, but most were still susceptible to the polymyxin antibiotic colistin. The Origin of SuperBug In early August 2010 a chemical compound GSK 299423, was found to significantly fight against antibiotic-resistant bacteria by making such bacteria unable to reproduce, citing a likely treatment to the NDM-1 strain. On August 21, 2010 Ontario, Canada had it?s first confirmed case of the "superbug" in Brampton. There have been other confirmed cases in British Columbia and Alberta. Indian response The Indian health ministry has disputed the conclusion of the August 2010 Lancet study that the gene originated in India or Pakistan, describing this conclusion as "unfair" and stating that Indian hospitals are perfectly safe for treatment. Indian politicians have described linking this new drug resistance gene to India as "malicious propaganda" and blamed multinational corporations for what they describe as selective malignancy. A Bharatiya Janata Party politician has instead argued that the journal article is bogus and represented an attempt to scare medical tourists away from India. The Indian Ministry of Health released a statement "strongly refut[ing]" naming the enzyme "New Delhi". The primary author of the 2010 Lancet study, who is based in the University of Madras, has stated that he does not agree with the part of the article that advises people to avoid elective surgeries in India. In contrast, an editorial in the March 2010 issue of the Journal of Association of Physicians of India blamed the emergence of this gene on the widespread misuse of antibiotics in the Indian healthcare system, stating that Indian doctors have "not yet taken the issue of antibiotic resistance seriously" and noting little control over the prescription of antibiotics by doctors and even pharmacists.The Times of India states that there is general agreement among experts that India needs both an improved policy to control the use of antibiotics and a central registry of antibiotic-resistant infections. In August 2010, the first reported death due to a bacteria expressing the NDM-1 enzyme was recorded as a Belgian man who had become infected, while being treated in a hospital in Pakistan. He died despite being administered colistin, a powerful antibiotic. A doctor involved in his treatment said, "He was involved in a car accident during a trip to Pakistan. He was hospitalized with a major leg injury and then repatriated to Belgium, but he was already infected". New Update Gram-negative Enterobacteriaceae with resistance to carbapenem conferred by New Delhi metallo-?-lactamase 1 (NDM-1) are potentially a major global health problem. We investigated the prevalence of NDM-1, in multidrug-resistant Enterobacteriaceae in India, Pakistan, and the UK. Methods Enterobacteriaceae isolates were studied from two major centres in India - Chennai (south India), Haryana (north India) - and those referred to the UK's national reference laboratory. Antibiotic susceptibilities were assessed, and the presence of the carbapenem resistance gene blaNDM-1 was established by PCR. Isolates were typed by pulsed-field gel electrophoresis of XbaI-restricted genomic DNA. Plasmids were analysed by S1 nuclease digestion and PCR typing. Case data for UK patients were reviewed for evidence of travel and recent admission to hospitals in India or Pakistan. Findings We identified 44 isolates with NDM-1 in Chennai, 26 in Haryana, 37 in the UK, and 73 in other sites in India and Pakistan. NDM-1 was mostly found among Escherichia coli (36) and Klebsiella pneumoniae (111), which were highly resistant to all antibiotics except to tigecycline and colistin. K pneumoniae isolates from Haryana were clonal but NDM-1 producers from the UK and Chennai were clonally diverse. Most isolates carried the NDM-1 gene on plasmids: those from UK and Chennai were readily transferable whereas those from Haryana were not conjugative. Many of the UK NDM-1 positive patients had travelled to India or Pakistan within the past year, or had links with these countries. Interpretation The potential of NDM-1 to be a worldwide public health problem is great, and co-ordinated international surveillance is needed.
|

 Forum
Forum Sitemap
Sitemap Contact
Contact



















 Petechial fever
Petechial fever
